The Role Of The Universities In The Struggle Against Inequity
The Role Of The Universities In The Struggle Against Inequity / INJUSTICE IN HEALTH SYSTEMS
Prof. Dr. Zafer Öztek MD
Hacettepe University
Faculty of Medicine
Department of Public Health
INTRODUCTION
Equity in health implies that health is a human right and everyone should have the equal opportunity to attain their full health potential and that no one should be disadvantaged from achieving this potential. The term inequity refers to differences in health which are not only unnecessary and avoidable but, in addition, are considered unfair and unjust (1).
Health is not equally distributed throughout the world and inequity is a problem of almost every nation(2). Therefore it is a crucial responsibility of all states to tackle with this issue. This approach was stated in the Declaration of Alma-Ata (item 2) as “the existing gross inequity in the health status of the people particularly between developed and developing countries as well as within countries is politically, socially and economically unacceptable and is, therefore, of common concern to all countries.” (3)
Since the days of Hippocrates, health inequities and the role of social and environmental factors in the determination of marked differences in health status have been well recognized(4). Reasons for disparities in access to health care and in the quality of care are many, but they can be listed as below (5):
- Lack of regular source of care (Poor health care organization; Scarcity of providers; Lack of diversity in health care workforce)
- Financial factors (Lack of financial resources; Lack of insurance coverage; The health care financing system)
- Structural barriers (Poor transportation; Long waiting lists etc)
- Cultural and personal factors (Age; Health literacy; Communication problems)
- Provider discrimination (Gender; Ethnicity; Minority groups; etc)
- Legal barriers (Immigrants; etc)
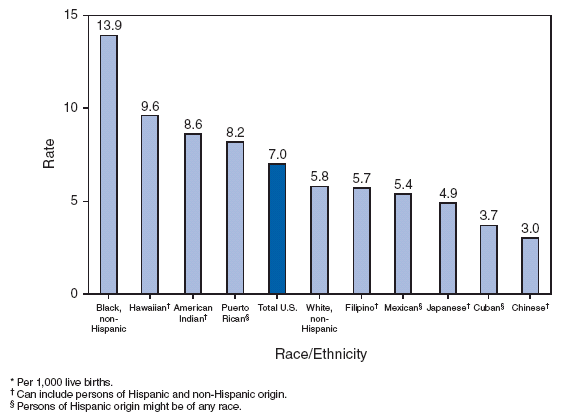
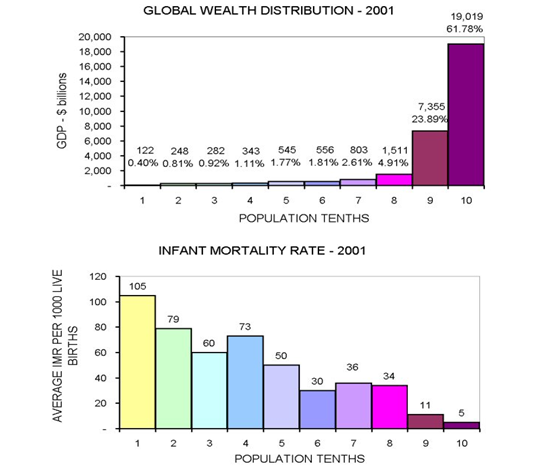
Many criteria can be used for the evaluation of inequality in health care and its impact on people’s health. Infant and child mortality rates are good outcomes of health care which also reflect the inequality problem. As it is seen in the table and figures below, the infant mortality rates (IMR) and under 5 mortality rates differ between socioeconomic, regional and ethnic groups.
Table 1 : Infant Mortality in the Main Regions of the World in 2005
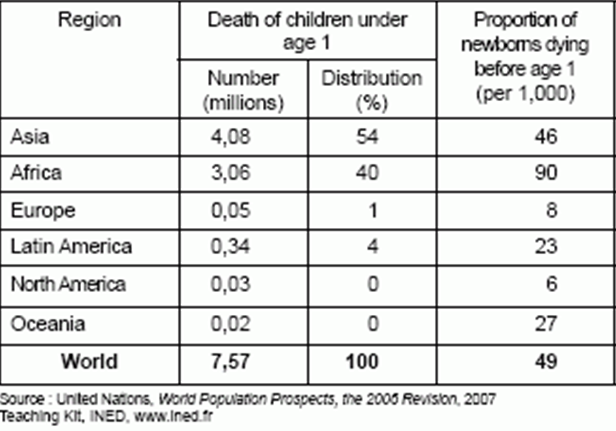
Figure 1 : Under 5 Mortality : Differences Between Rich and Poor
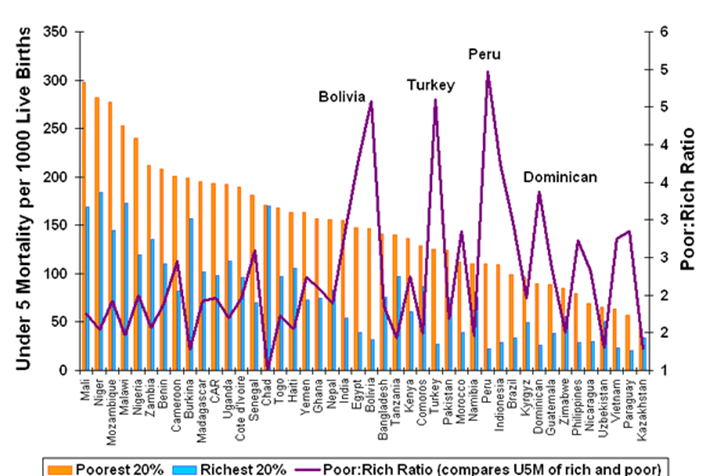
Figure 2 : Infant Mortality Rates by Selected Racial / Ethnic Populations
in United States in 2002
Figure3 : Relation Between Wealth and Infant Mortality
SOLUTIONS
The Alma-Ata Declaration addressed the basic strategy for tackling the inequity problem in health in its fifth item: “Governments have a responsibility for the health of their people which can be fulfilled only by the provision of adequate health and social measures. A main social target of governments, international organizations and the whole world community in the coming decades should be the attainment by all people of the world by the year 2000 of a level of health that will permit them to lead a socially and economically productive life. Primary health care is the key to attaining this target as part of development in the spirit of social justice.” (3)
Recognizing the special needs of those who are least able, for geographical, political, social, or financial reasons, to take the initiative in seeking health care, and expressing great concern for those who are the most vulnerable or at greatest risk the Declaration of Alma-Ata recommended (recommendation No.8) that, as part of total coverage of populations through primary health care, high priority be given to the special needs of women, children, working populations at high risk, and the underprivileged segments of society, and that the necessary activities be maintained, reaching out into all homes and working places to identify systematically those at highest risk, to provide continuing care to them, and eliminate factors contributing to ill health (3).
Related with the Alma-Ata Declaration, the health for all policy framework for the WHO European Region has formulated 21 targets for the 21st century (6). The second target of this document is specifically towards the reduction of inequality in health:
Target 2: By the year 2020, the health gap between socioeconomic groups within countries should be reduced by at least one fourth in all member states, by substantially improving the level of health of disadvantaged groups. In particular,
- The gap in life expectancy between socioeconomic groups should be reduced by at least 25 %;
- The values for major indicators of morbidity, disability and mortality in groups across the socioeconomic gradient should be more equitably distributed;
- Socioeconomic conditions that produce adverse health effects, notably differences in income, educational achievement and access to the labor market, should be substantially improved;
- The proportion of the population living in poverty should be greatly reduced;
- People having special needs as a result of their health, social or economic circumstances should be protected from exclusion and given easy access to appropriate care.
Sectors’ responsibilities
Increased equity in health care leads to public health gain and thus helps social development, higher productivity and sustained economic growth. It is therefore imperative that public policies address the root causes of socioeconomic inequities and those fiscal, educational and social policies are designed to ensure a sustained reduction of health inequalities. All sectors of society should assume responsibility for the reduction of social and gender inequities, and the alleviation of their consequences on health(7).
Role of universities
The universities and other schools have a special role in minimizing inequity in health and make great input in raising the health status of people.
The Alma-Ata Declaration has recommended that all health personnel including physicians, traditional medical practitioners and all other health personnel should be trained and motivated to serve the community and their training programs should include field activities so that they should be urged to work in underserved areas at least in their early career (3, 8). The preparation of health personnel needs to be strengthened in terms of relevance to health services and people’s health needs and demands (9). Universities and other training institutions have key roles to play in addressing these issues.
All health professionals have a special responsibility to respond to the struggle for better health for disadvantaged groups (10). This responsibility should fall not only on individuals but also on institutions concerned with the provision of health care and education of those who will work in the health field. Academic centers traditionally have large concentrations of resources, particularly those relating to intellectual capital and also rely on the local community for financial and intangible support. They have the means and the social obligation to improve health at a minimal level in the communities in which they are located(11). It is suggested that the contribution to lessening health inequity should be seen as an integral part of undergraduate medical education and institutions that provide such courses(12).
There are a number of ways in which schools of medicine can promote health equity(13):
- Selection of students in medical programs
It is important that students are selected from a variety of backgrounds for reasons of social equity as well as to increase the probability that the delivery of healthcare is more likely to be culturally and socially appropriate (11). There is some evidence to suggest that students who are accepted to medical schools from minority groups such as Indigenous and rural born students and students who come from socio-economically disadvantaged areas are more likely to understand the needs of these populations and may ultimately practice in similar environments (14, 15).
- Content in the curriculum
Students’ perceptions of how health care should be provided are potentially influenced by the curriculum content. In order to make students to be aware of inequity and encourage them to practice in a way which would overcome health inequities the content of the curriculum is essential. The core curriculum and the training material should give the students the opportunity to explore other areas outside of core during their undergraduate experience. One such experience could involve providing undergraduate students with an opportunity of becoming health activists (16).
- Model health service delivery to overcome health inequity
University medical programs are able to play a role in demonstrating and helping to provide access for the disadvantaged groups. The majority of medical clinicians who teach in university environments have traditionally been based in large teaching hospitals. However, establishing university supported physicians and health care teams outside the teaching hospital has the potential, not only to improve the quality of care offered in these environments, but also to serve as an important role model for undergraduate students (17). It is not only necessary to provide increased content in the undergraduate program but also to demonstrate a commitment by faculty academics to work with and assist disadvantaged groups. Such demonstrations may involve the establishment of clinics operating in communities where there is a high level of disadvantage, but is also reflected in individuals within the medical and other health undergraduate programs being prepared to adopt a high profile in lobbying for the betterment of health for those who are disadvantaged. They may do this through public programs, political activity, and formation of groups who have, as their focus, attempts to redress the current imbalance in health status (13).
- Proportional numbers and interests of academic faculty role models
There is a need to reflect, in the proportional number of employed university staff in medical schools, a commitment to issues relating to health inequalities. This can be reflected in the academics titles as well as their teaching and research interests(13).
- Research and consultancy to policy makers
For making appropriate and sustainable decisions the decision makers need reliable evidences. Such evidences can be served by academicians through community based service researches and pilot studies undertaken in the research and training areas of the universities or in the areas of disadvantaged groups. Academicians can also assist the decision makers for evaluating their interventions and guide them for better models for realizing an equitable health care.
Role of other schools
Social responsibility can be demonstrated at young ages. Therefore, school boards of primary and secondary grades should incorporate social responsibility as part of their curriculum (18). Defending human rights is an important aspect in these curricula. In the lessons it is very important to teach the young students that health is a human right and every citizen should have the equal chance of reaching health services and getting care as much as they need. It is the governments responsibilities to make the youth of their nation be aware, that inequities should be unacceptable not only in their country but in the rest of the world.
Schools should also take initiative in running “healthy school programs” and creating the children and young people an understanding of risk and encouraging them to have health literacy to make healthy choices (19). These choices would deal healthy eating, physical activity, safe sexual relations, avoiding smoking and drug use, which will help them using health services appropriately, preventing themselves from diseases and saving their health.
REFERENCES
- Health for all targets: the health policy for Europe, WHO Regional Office for Europe, European Health for All Series, No. 4, Copenhagen, 1993
- Gunning-Schepers LJ, Spruit IP, Krijnen JH. Socio economic inequalities in health, Ministry of Welfare, Health and Cultural Affairs, The Hague, 1989.
- Primary Health Care – Report of the International Conference on Primary Health Care, Alma-Ata, USSR, 6-12 September 1978, World Health Organization, Geneva, 1978
- Casas-Zamora,JA, Ibrahim S. Confronting health inequity: The global dimention, Am. J.PH, Vol 94, No 12, 2004.
- Fryer GE, Dovey SM, Green LA The importance of having a usual source of health care, Am Family Physician 62 (2000): 477
- Health 21: Health for all in the 21st century, WHO Regional Office for Europe, European Health for All Series No. 6, Copenhagen, 1999.
- An introduction to the health for all policy framework for the WHO European Region, European Health for All Series No. 5, World Health Organization Regional Office for Europe, Copenhagen, 1998.
- Formulating strategies for health for all by the year 2000, World Health Organization, Geneva, 1979.
- From Alma-Ata to the year 2000- Reflections at the midpoint, World Health Organization, Geneva, 1988.
- Jotkowitz AB, Glick S, Porath A. A physician charter on medical professionalism: A challenge for medical education. Eur J Intern Med2004; 15(1)5–9
- Nickens HW, Ready TP, Petersdorf RG. Project 3000 by 2000. Racial and ethnic diversity in US medical schools. New Eng J Med1994; 331(7)472–476
- Betancourt JR. The Institute of Medicine report “Unequal Treatment”: implications for academic health centers. Mt Sinai J Med2004; 71(5)314–321
- Sanson-Fisher RW, Williams N., Outram S. Health inequilaties: the need for action by schools of medicine, Medical Teacher 2008, Vol. 30, No. 4, Pages 389-394
- Garvey G, Rolfe IE, Pearson S. Agents for social change: the role of universities in graduating Aboriginal and Torres Strait Islander doctors. Focus Health Prof Edu2000; 2(2)18–27
- Rolfe IE, Pearson S, O’Connell d, Dickinson JA. Findings solutions to the rural doctor shortage: the role of undergraduate medical education versus selection at Newcastle. Austr&N Z J Med1995; 25: 512–517
- Dodson JA, Keller AS. Medical student care of indigent population. J Am Med Assoc2004; 291(1)121–128
- Cashman SB, Hale JF, Candib LM, Nimiroski TA, Brookings DR. Applying service learning through a community-academic partnership: depression screening at a federally funded community health center. Edu Health2004; 17(3)313–322
- Tam G., Teaching health equity and global responsibility to the next generation – a school project, University of Ottawa, Canada.
- Health inequalities – Third report of session 2008-09, House of Commons Health Committee, London, 15 March 2009.